
Adenomyosis is a condition of the uterus in which endometriotic tissue is found within the muscular walls of the uterus. Adenomyosis can be focal or diffuse. Focal adenomyosis also referred to as an adenomyoma, is when a tumorous growth of endometriotic tissue forms inside the muscular uterine walls. More commonly, however, diffuse areas of endometriotic tissue are dispersed through the uterine muscle, most often affecting the posterior (back) wall of the uterus, which can become thickened as a result.
What are the symptoms of adenomyosis?
 Adenomyosis can result in abnormal uterine bleeding (typically heavy and prolonged menstrual flows) and/or severe uterine cramping – “killer cramps.” Sometimes adenomyosis may not cause any symptoms at all. Patients who suffer from adenomyosis often report severe centralized cramping pain that worsens during the menstrual flow and may radiate up to the belly button and/or down to the lower back and into the buttocks and thighs. One reason why pain may radiate is because the uterus is innervated by nerves that run along the uterine ligaments, which lead upwards toward the umbilicus and downwards to the lower back. Some patients have such severe uterine pain that over time they develop second-degree burns over their abdominal area from the prolonged use of heating pads in an effort to sooth their debilitating cramps.
Adenomyosis can result in abnormal uterine bleeding (typically heavy and prolonged menstrual flows) and/or severe uterine cramping – “killer cramps.” Sometimes adenomyosis may not cause any symptoms at all. Patients who suffer from adenomyosis often report severe centralized cramping pain that worsens during the menstrual flow and may radiate up to the belly button and/or down to the lower back and into the buttocks and thighs. One reason why pain may radiate is because the uterus is innervated by nerves that run along the uterine ligaments, which lead upwards toward the umbilicus and downwards to the lower back. Some patients have such severe uterine pain that over time they develop second-degree burns over their abdominal area from the prolonged use of heating pads in an effort to sooth their debilitating cramps.
Are endometriosis and adenomyosis related?
There does appear to be a strong association between these two conditions. A subset of women who suffer from endometriosis will also, unfortunately, have adenomyosis to varying degrees and often a clinical challenge in resolving a patient’s pain is to successfully differentiate between the symptoms of endometriosis and adenomyosis. This is why it is important that your doctor assesses both the uterus and the tissue around the uterus separately in order to discern the source of your pain.
Can anything be done about adenomyosis?
Several treatments for adenomyosis are available, both conservative (organ-preserving) and radical (organ removal). Conservative treatments include pain management with non-prescription and prescription pain medications and the use of hormone therapies to suppress the menstrual cycle and either shorten or temporarily stop the menstrual flow. Sometimes a surgical procedure called a presacral neurectomy (PSN) will be performed to sever the nerves that innervate the uterus with the aim of alleviating uterine cramping. This procedure may not be especially effective in patients with adenomyosis however as the disease may result in localized inflammation that extends beyond the uterus itself, affecting surrounding extra-uterine tissues. A PSN has no effect on these surrounding tissues and therefore a portion of the patient’s pain may persist despite the procedure. A PSN also has no effect on abnormal uterine bleeding. In those patients who do not have future plans for fertility or who have completed childbearing, a hysterectomy may be considered. Hysterectomy is the only definitive (curative) treatment for diffuse adenomyosis. If a patient has an adenomyoma (focal adenomyosis) it may be possible to surgically remove the adenomyoma, rather like one might remove a fibroid, while preserving the rest of the uterus. This will depend on the size of the adenomyoma, it’s location and on the skill of the surgeon.
How is adenomyosis diagnosed?
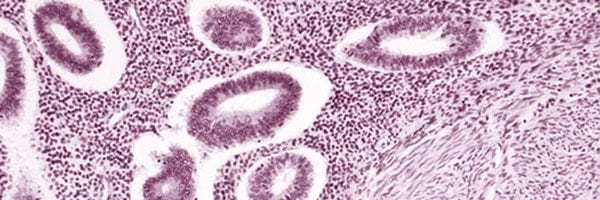
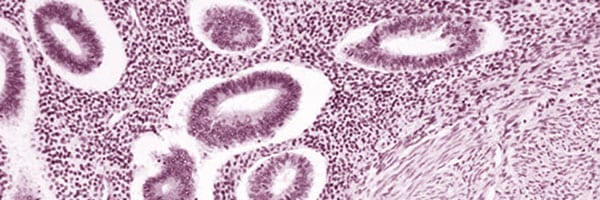
 The only definitive method of diagnosing adenomyosis is by obtaining a biopsy of the diseased tissue and having a pathologist inspect it under the microscope for the presence of endometriotic tissue. While this may be readily possible if a patient has an adenomyoma, in the case of diffuse adenomyosis, obtaining a biopsy of diseased tissue may not be feasible until after hysterectomy (it would be akin to searching for a needle in a haystack). Endometrial biopsies may confirm a diagnosis of adenomyosis in some cases if the biopsy is sufficiently deep but failing to confirm the diagnosis via this test does not exclude adenomyosis and this is not a routine test for adenomyosis but may be undertaken to exclude other possible causes of abnormal uterine bleeding. In most cases, the diagnosis is suspected based on the patient’s symptoms and on the findings from imaging studies (ultrasounds, CT and/or MRI). Sometimes the uterus may be found to be enlarged and have a “boggy” consistency during laparoscopy, raising a suspicion of possible adenomyosis. If diffuse adenomyosis is subtle, however, it may not be apparent on imaging nor at surgery. The absence of any telltale signs should not exclude adenomyosis as a possible source of uterine pain and the patient’s debilitating uterine symptoms still need to be addressed.
The only definitive method of diagnosing adenomyosis is by obtaining a biopsy of the diseased tissue and having a pathologist inspect it under the microscope for the presence of endometriotic tissue. While this may be readily possible if a patient has an adenomyoma, in the case of diffuse adenomyosis, obtaining a biopsy of diseased tissue may not be feasible until after hysterectomy (it would be akin to searching for a needle in a haystack). Endometrial biopsies may confirm a diagnosis of adenomyosis in some cases if the biopsy is sufficiently deep but failing to confirm the diagnosis via this test does not exclude adenomyosis and this is not a routine test for adenomyosis but may be undertaken to exclude other possible causes of abnormal uterine bleeding. In most cases, the diagnosis is suspected based on the patient’s symptoms and on the findings from imaging studies (ultrasounds, CT and/or MRI). Sometimes the uterus may be found to be enlarged and have a “boggy” consistency during laparoscopy, raising a suspicion of possible adenomyosis. If diffuse adenomyosis is subtle, however, it may not be apparent on imaging nor at surgery. The absence of any telltale signs should not exclude adenomyosis as a possible source of uterine pain and the patient’s debilitating uterine symptoms still need to be addressed.
Can adenomyosis affect women of any age?
Adenomyosis is often considered to be a disease that primarily affects middle-aged and older women (30s onwards), especially women who have previously given birth. This bias could, however, be due to the fact that usually only women who have completed their families undergo hysterectomy for the treatment of their uterine pain. Given adenomyosis can almost always only be confirmed via biopsy following hysterectomy, this inevitably leads to the impression that the disease only affects women who have completed childbearing. Furthermore, the symptoms of endometriosis may often overshadow the symptoms of adenomyosis in the early course of the disease, giving the impression that its onset is later. In reality, however, both endometriosis and adenomyosis can affect women of any age, including teenagers.



i have suffered with endometriosis and cistitus for many years i’ve had an operation to remove a endometrioma and currently taking hormone injections…i needto know how long i can continue with these injections i am 45 had have been in treatment for 8 years.
I am a 34 –year-old girl who suffers from adenomyosis. I am single and virgin. Doctors in my country recommended hysterectomy. I have a heavy and long bloodshed during my menstrual period. Between two periods I have bloodshed too and I suffer from extreme fatigue, depression.
I used these medicals during 6 years 🙁 But no work)
Trancid acid-mefenamic- duphaston- ibuprophen- dipherelin SR 3.75 –decapeptyle – contraceptive LD-
I had laparoscopy-MRI –Sonography .My laparoscopy (5 years ago) diagnosis was PCO.
Because I am virgin I cannot use Mirena IUD.
This is my latest sonography:
Uterus size: 129*70*106 mm
Abnormal nodular echogenicity contain small hypoechoic foci can be seen.
Adenomyosis can be recommended.
Endometer diameter is normal: 3.9mm
Inmens phase and regular.There is no polipoid .
Ovary size is normal.
Right ovary size: 35*24mm
Left ovary size: 34*21mm
CX and vagina is normal.
No abnormal fluid of douglus pouch is seen.